Makindo Medical Notes.com |
|
|---|---|
| Download all this content in the Apps now Android App and Apple iPhone/Pad App | |
| MEDICAL DISCLAIMER:The contents are under continuing development and improvements and despite all efforts may contain errors of omission or fact. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice by healthcare workers or laypeople. It is for educational purposes only. Please adhere to your local protocols. Use the BNF for drug information. If you are unwell please seek urgent healthcare advice. If you do not accept this then please do not use the website. Makindo Ltd | |
Sarcoidosis
-
| About | Anaesthetics and Critical Care | Anatomy | Biochemistry | Cardiology | Clinical Cases | CompSci | Crib | Dermatology | Differentials | Drugs | ENT | Electrocardiogram | Embryology | Emergency Medicine | Endocrinology | Ethics | Foundation Doctors | Gastroenterology | General Information | General Practice | Genetics | Geriatric Medicine | Guidelines | Haematology | Hepatology | Immunology | Infectious Diseases | Infographic | Investigations | Lists | Microbiology | Miscellaneous | Nephrology | Neuroanatomy | Neurology | Nutrition | OSCE | Obstetrics Gynaecology | Oncology | Ophthalmology | Oral Medicine and Dentistry | Paediatrics | Palliative | Pathology | Pharmacology | Physiology | Procedures | Psychiatry | Radiology | Respiratory | Resuscitation | Rheumatology | Statistics and Research | Stroke | Surgery | Toxicology | Trauma and Orthopaedics | Twitter | Urology
Related Subjects: |Idiopathic Pulmonary Fibrosis |Diffuse Parenchymal Lung disease |Asbestos Related Lung disease |Sarcoidosis |Coal Worker's Pneumoconiosis |Silicosis |Farmer's Lung |Cryptogenic Organising Pneumonia (COP-BOOP) |Extrinsic Allergic alveolitis (Hypersensitivity) |Byssinosis |Pneumoconiosis |Cor Pulmonale
Sarcoidosis is a systemic inflammatory disease characterized by the formation of non-caseating granulomas in various organs. The exact cause is unknown, but it is thought to result from an exaggerated immune response to an unknown antigen. The disease most commonly affects the lungs and lymph nodes but can involve any organ system.
About
- Non caseating granulomatous systemic disease
- Protean manifestations affecting many organs
Epidemiology
- Blacks > whites. Females >Males. Onset Age 20-40
- African-Americans and people of Northern European descent
The hallmark of sarcoidosis is the formation of non-caseating granulomas, which are clusters of immune cells, primarily macrophages and T lymphocytes. These granulomas can form in various organs, leading to tissue inflammation and damage. The exact trigger for this immune response is unknown, but it is believed to involve genetic susceptibility and environmental factors, such as infectious agents or occupational exposures
Aetiology
- Cutaneous anergy - lack of a skin reaction to various antigens e.g. tuberculin
- Diminished cell-mediated immune response to antigens
- Reduced lymphocytes and low circulating T cells as they are sequestered in lungs
- Mildly increased B cells in peripheral blood and increased bronchial CD4 cells
Clinical
- Cough, dyspnoea, and chest pain are common when the lungs are affected.
- Erythema nodosum - a painful, red skin rash, often occurs on the shins.
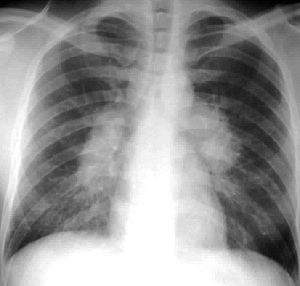
- Arthralgia, Bilateral hilar lymphadenopathy
- Chronic - worse prognosis - Gradual increasing dyspnoea, Pulmonary fibrosis and systemic complications
- Asymptomatic disease in 30% with only CXR changes
- Arthritis: Feet and hands and large joints may be affected too
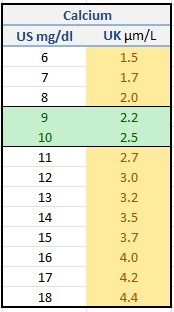
- General: Lymphadenopathy, Hypercalcaemia in less than 10% and rarely severe.
- Eye: Uveitis, characterized by eye pain and redness and visual loss
- Cardiac: Heart block, VT, ECG changes, Cardiomyopathy (v rare) and CCF may be seen.
- Uveoparotid fever: Heerfordt's syndrome - Uveitis + Parotids enlarged + VIIth palsy + Fever
- Lofgren's syndrome: BHL + EN + arthritis/arthralgia + fever
- Skin: 25%. Erythema nodosum, Lupus pernio (red/blue nose), Nodules, scar infiltration
- CNS: Chronic granulomatous meningitis, Fits, Peripheral/cranial neuropathy
- Endocrine: Hypothalamic lesions - diabetes insipidus and Hypercalcaemia
- Haematological: Generalised lymphadenopathy, low CD4 count
- Liver: granulomas on biopsy and mild deranged LFT's
- Bone: cystic lesions can develop
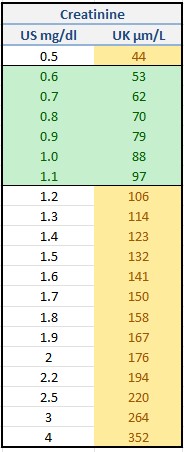
- Renal: interstitial nephritis, Glomerulonephritis, Renal stones (high Calcium)
- Often the patients are female of childbearing age and pregnancy usually improves symptoms.
 Sarcoid
Sarcoid
 Sarcoid
Sarcoid
 Sarcoid
Sarcoid
 Sarcoid
Sarcoid
Stages of Pulmonary Sarcoidosis
- Stage I: Bilateral hilar lymphadenopathy without pulmonary infiltrates.
- Stage II: Bilateral hilar lymphadenopathy with pulmonary infiltrates.
- Stage III: Pulmonary infiltrates without hilar lymphadenopathy.
- Stage IV: Pulmonary fibrosis with or without honeycombing.
Differential
- Tuberculosis - check smear for open TB and tuberculin testing
- Lymphoma - do HRCT
- Lung cancer with localised spread
Investigations
- The ESR and CRP may be elevated with active disease
- Raised serum ACE: from epithelioid cells of the granulomas
- Raised 1,25(OH)2 D3 and mild hypercalcaemia in only 10%
- Tuberculin tests are usually negative
- Bronchoscopy - Cobble stoning of mucosa and lavage shows an increased CD4:CD8 T cell ratio
- Transbronchial Biopsies - Non-caseating granulomata on biopsy
- Liver Biopsies - Non-caseating granulomata on biopsy
- ECG or 24 hr tape: heart blocks
- Kveim test: injection of splenic extract from a sarcoid patient injected intradermally and then biopsied but now cannot be done with risks of infections.
- Immunoglobulins: elevated hypergammaglobulinaemia
- Exclude open (smear-positive) TB before formal lung function tests or risks contaminating the equipment.
- Reduced transfer factor, Restrictive (small lung) PFT's and reduced DLCO
- High-resolution CT: BHL, fibrosis - ground glass appearance suggests active disease which may be steroid responsive
- Gallium-67 scan: The "panda sign" (localization in the lacrimal and salivary glands, giving a typical panda appearance to the face) is suggestive of sarcoidosis
Staging and Prognosis based on the CXR findings
- 0: CXR normal bit may have EN and arthralgia. Most cases resolve in 1 year
- I: BHL with no lung infiltrates 80% resolve spontaneously. EN and arthralgia.
- II: BHL + pulmonary infiltrate 50% resolve spontaneously. Breathlessness and cough.
- III: No BHL but Pulmonary infiltrates 10-25% resolve
- IV: Advanced fibrosis honeycombing, hilar retraction, bullae, cysts, emphysema. 0% resolve. Cor pulmonale
Prognostic indicators
- Good: younger, erythema nodosum
- Poor: Age > 40, Afro-Caribbean, Continuous symptoms over 6 months, Lupus pernio, Involvement of over 3 organs, CXR stages III-IV,
Management
| Treatment Option | Description |
|---|---|
| Observation | Appropriate for patients with asymptomatic or mild disease. Supported by regular clinical evaluation and imaging (e.g., CXR, pulmonary function tests). Many cases undergo spontaneous remission. |
| Corticosteroids | First-line treatment for symptomatic sarcoidosis or significant organ involvement. Corticosteroids: Prednisolone 20-30 mg od for 6 weeks and then a reduced dose. Dosage and duration depend on the severity of disease and response to treatment. Long-term use may cause side effects such as weight gain, osteoporosis, and diabetes. |
| Immunosuppressive Agents | For those who do not respond to corticosteroids or as steroid sparing agents. Methotrexate 10-20 mg/week, Azathioprine (50-150 mg/day), and Mycophenolate Mofetil. Control the immune response and reduce granuloma formation. Monitor for bone marrow suppression and liver toxicity. |
| Antimalarial Drugs | Hydroxychloroquine or Chloroquine can be effective, particularly for skin, joint, or hypercalcemia-related manifestations. They modulate the immune response. Ocular toxicity is a potential side effect, requiring regular ophthalmologic monitoring. |
| Biologic Agents | Considered in refractory cases where conventional therapies fail. TNF-alpha inhibitors (e.g., Infliximab, Adalimumab) are commonly used. These drugs target specific components of the immune system, reducing inflammation. Increased risk of infections; screening for latent tuberculosis is required before initiating therapy. |
| Symptomatic Treatment | Treatment aimed at managing specific symptoms, such as cough, pain, or fatigue. Inhaled bronchodilators or corticosteroids may be used for respiratory symptoms. NSAIDs or analgesics for joint pain or arthritis. |
| Organ-Specific Interventions |
Cardiac involvement: May require pacemaker or implantable cardioverter-defibrillator (ICD) for arrhythmias.
Ocular sarcoidosis: Treated with topical or steroids. Neurosarcoidosis: Aggressive immunosuppressive therapy with steroids and other agents. |
| Lifestyle Modifications | Smoking cessation is crucial for lung health. Encourage regular, moderate exercise. Maintain a balanced diet |
| PLEASE NOTE LEGAL ADVICE: The contents are under continuing development and improvements and may contain errors of omission or fact. Feedback vital and always welcome at drokane at gmail.com. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice. It is only for educational purposes. Please adhere to your local protocols. If you are unwell please seek healthcare advice from your doctor. This does not replace senior or specialist advice. If you do not accept this then please do not use the website. If you need medical advice, please consult a doctor or other appropriate medical professional. If you are a medical professional and you need advice then speak to your senior or colleagues. |