Makindo Medical Notes.com |
|
|---|---|
| Download all this content in the Apps now Android App and Apple iPhone/Pad App | |
| MEDICAL DISCLAIMER:The contents are under continuing development and improvements and despite all efforts may contain errors of omission or fact. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice by healthcare workers or laypeople. It is for educational purposes only. Please adhere to your local protocols. Use the BNF for drug information. If you are unwell please seek urgent healthcare advice. If you do not accept this then please do not use the website. Makindo Ltd | |
Case #10 Weakness
-
| About | Anaesthetics and Critical Care | Anatomy | Biochemistry | Cardiology | Clinical Cases | CompSci | Crib | Dermatology | Differentials | Drugs | ENT | Electrocardiogram | Embryology | Emergency Medicine | Endocrinology | Ethics | Foundation Doctors | Gastroenterology | General Information | General Practice | Genetics | Geriatric Medicine | Guidelines | Haematology | Hepatology | Immunology | Infectious Diseases | Infographic | Investigations | Lists | Microbiology | Miscellaneous | Nephrology | Neuroanatomy | Neurology | Nutrition | OSCE | Obstetrics Gynaecology | Oncology | Ophthalmology | Oral Medicine and Dentistry | Paediatrics | Palliative | Pathology | Pharmacology | Physiology | Procedures | Psychiatry | Radiology | Respiratory | Resuscitation | Rheumatology | Statistics and Research | Stroke | Surgery | Toxicology | Trauma and Orthopaedics | Twitter | Urology
Related Cases: |Case #1 Potassium |Case #2 Calcium |Case #3 Calcium |Case #4 Glucose |Case #5 Shakes |Case #6 Weakness |Case #7 Headache |Case #8 Weakness |Case #9 Weakness |Case #10 Weakness |Case #11 Weak face |Case #12 Weak eyes |Case #13 Shakes |Case #14 Confusion |Case #15 Headache |Case #16 Breathless |Case #17 Unconscious |Case #18 Breathless |Case #19 Weakness |Case #20 Breathless
Mary is an 80-year-old lady who developed some altered speech whilst out on a day trip shopping from Chelmsford to Brighton. She was found to have right face, arm and leg weakness and has difficulty with speech and language. She has been brought in by paramedics. She complains of a headache. The time of onset was 5.20 pm. She was FAST positive for speech and arm weakness.
Her ECG shows AF. The paramedics think she is worse than when they picked her up. She has diabetes and her BM is 8.9. She has a long history of hypertension and the BP is 200/70 mmHg. She has an NIHSS of 15. It is now 6 pm. You attend the stroke call with the specialist nurse. She has no local hospital records as she is away from home.
1. Do you think this will be an ischaemic or haemorrhagic stroke
2. What is the most important test
3. Click to see the CT scan
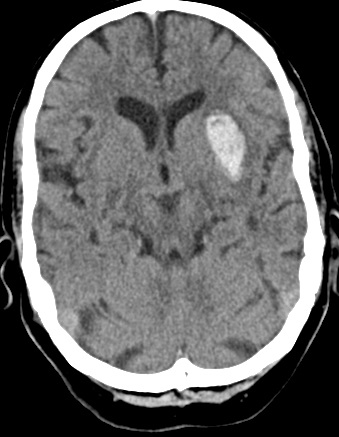
4.Intepret the Scan
5. What actions should you consider
ABC and admission to HASU. Consider ITU if GCS < 9. Check clotting and platelets. The AF concerns us that the patient may be on Warfarin and a raised INR would suggest this. Try and check the patient's medications as they may also be on a DOAC. These would need their specific reversal agent. Stop any Clopidogrel or Aspirin. Monitor and Lowering BP cautiously using local protocols. Monitoring BMs as diabetic. Swallow assessment. Contacting family or those important to the patient to let them know the situation but also to get as much background history as possible and baseline functional status and any views expressed on resuscitation.
6. What are the commonest causes of ICH in this age group
- Chronic hypertension
- Cerebral amyloid angiopathy
- Anticoagulants e.g. on warfarin
- Trauma
- Bleeding associated with a tumour
- Arteriovenous Malformation or Cavernoma
7. The INR is 2.2. What actions should you consider
References
| PLEASE NOTE LEGAL ADVICE: The contents are under continuing development and improvements and may contain errors of omission or fact. Feedback vital and always welcome at drokane at gmail.com. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice. It is only for educational purposes. Please adhere to your local protocols. If you are unwell please seek healthcare advice from your doctor. This does not replace senior or specialist advice. If you do not accept this then please do not use the website. If you need medical advice, please consult a doctor or other appropriate medical professional. If you are a medical professional and you need advice then speak to your senior or colleagues. |