Makindo Medical Notes.com |
|
|---|---|
| Download all this content in the Apps now Android App and Apple iPhone/Pad App | |
| MEDICAL DISCLAIMER:The contents are under continuing development and improvements and despite all efforts may contain errors of omission or fact. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice by healthcare workers or laypeople. It is for educational purposes only. Please adhere to your local protocols. Use the BNF for drug information. If you are unwell please seek urgent healthcare advice. If you do not accept this then please do not use the website. Makindo Ltd | |
Case #9 Weakness
-
| About | Anaesthetics and Critical Care | Anatomy | Biochemistry | Cardiology | Clinical Cases | CompSci | Crib | Dermatology | Differentials | Drugs | ENT | Electrocardiogram | Embryology | Emergency Medicine | Endocrinology | Ethics | Foundation Doctors | Gastroenterology | General Information | General Practice | Genetics | Geriatric Medicine | Guidelines | Haematology | Hepatology | Immunology | Infectious Diseases | Infographic | Investigations | Lists | Microbiology | Miscellaneous | Nephrology | Neuroanatomy | Neurology | Nutrition | OSCE | Obstetrics Gynaecology | Oncology | Ophthalmology | Oral Medicine and Dentistry | Paediatrics | Palliative | Pathology | Pharmacology | Physiology | Procedures | Psychiatry | Radiology | Respiratory | Resuscitation | Rheumatology | Statistics and Research | Stroke | Surgery | Toxicology | Trauma and Orthopaedics | Twitter | Urology
Related Cases: |Case #1 Potassium |Case #2 Calcium |Case #3 Calcium |Case #4 Glucose |Case #5 Shakes |Case #6 Weakness |Case #7 Headache |Case #8 Weakness |Case #9 Weakness |Case #10 Weakness |Case #11 Weak face |Case #12 Weak eyes |Case #13 Shakes |Case #14 Confusion |Case #15 Headache |Case #16 Breathless |Case #17 Unconscious |Case #18 Breathless |Case #19 Weakness |Case #20 Breathless
John is a 62-year-old right-handed male. He was found collapsed in the town centre today. He was lying beside his car. He was conscious. He was FAST positive (abnormal speech and couldn't lift his right arm) and has been brought in by a paramedic crew and is now in the resus area of the ED. He is having his observations assessed. You have been pre alerted by the paramedics who are concerned that he is having a stroke and so go to meet him on arrival in the ED.
He has just arrived and the stroke nurse is arranging an urgent CT head. He is mute. The paramedics show you a parking ticket which shows that he entered the car park at 11.00 am. He is awake but there is no speech. He also does not appear to be moving his right arm and leg. He has a right facial weakness.
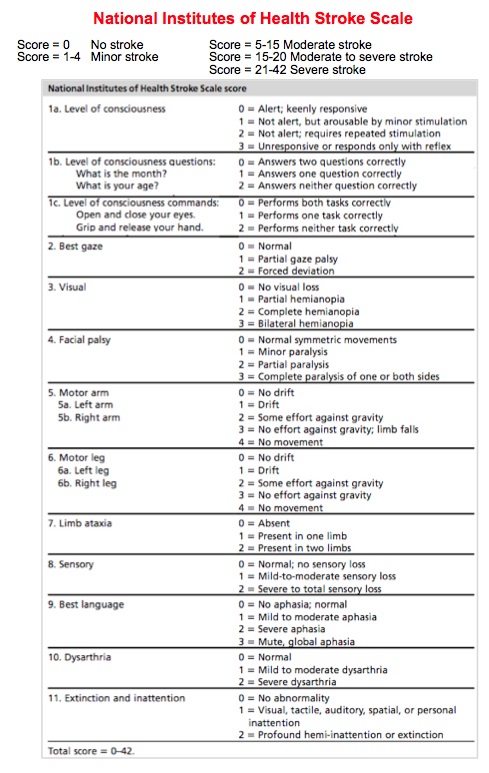
His BP is 150/80 mmHg and Pulse 80/min and O2 sats 95%. He does not appear to see visual stimuli on his right side. You quickly examine him and calculate his NIHSS score to be 15. The consultant advises get a CT and blood and is on her way. The team attempts to call his wife from details proved by paramedics.
Questions
1. What is the FAST test

2. What is NIHSS score
3. Why is contacting his wife so crucial
- His wife may know about past medical history e.g. a recent episode of GI bleeding or that patient is on Warfarin or that the patient has another condition that would be a contraindication to Thrombolysis.
- Wife or any witness may also be able to help with time of onset if there is uncertainty from other sources.
- Wife cannot give consent for anyone else but can support a best interest decision to thrombolyse a patient who lacks capacity. She may even have a Power of attorney for health and welfare and so be able to make decisions for the patient. Otherwise she can try to reflect what would be the patient's views.
- It is both kind and considerate to inform family as early as possible to come and emotionally support and be with the patient.
See Imaging
 >
>
- The CT shows a long clot/thrombus in the Left MCA M1
- The consultant checks inclusion and exclusion criteria
- The consultant checks that the BP is < 185/110 mmHg. It is 160/90 mmHg
- The consultant rechecks that the CT is compatible with ischaemic stroke
- The consultant speaks to his wife by phone and explains that he needs thrombolysis and risk and benefits
- He is treated in best interests as he lacks capacity due to loss of capacity due to aphasia
4. What are the usual signs of a blocked Left and Right MCA (dominant)
Blocked Left MCA
- Right sided weakness (hemiparesis) - right face/arm/leg
- Right sided hemisensory loss
- Right homonymous hemianopia
- Dysphasia
Blocked Right MCA
- Left sided weakness (hemiparesis) - left face/arm/leg
- Left sided hemisensory loss
- Left homonymous hemianopia
- Neglect/Inattention
5. His weight is 70 kg and Alteplase is given as 0.9 mg/kg. How much is given and how is it given
- His weight is 70 kg so Alteplase dose is therefore 0.9 mg/kg x 70 = 63 mg
- This is prepared by the stroke nurse specialist
- This is prescribed and 10% (6 mg) is given as a bolus and the remaining 90% is given through an infusion pump
- This will usually require the opening of 2 x 50 mg vials which are made up
- The remaining 90% ( 57 mg) is given as an infusion over 1 hour
- The patient must be closely monitored for complications with 15 minute obs
6. What is Alteplase
7. During the infusion he suddenly becomes less responsive and has a seizure . What would you do now.
- Immediately stop the Alteplase and check ABC and a set of observations.
- Start Oxygen. Check BM if hypoglycaemia possible.
- Escalate to the Medical Registrar or the stroke team.
- Once stabilised get a second CT scan to look for haemorrhage.
- Consider a phenytoin infusion if seizure persists or recures
- Continue frequent monitoring on the HASU
- If GCS < 9 then get anaesthetic review and discuss need for ventilatory support in an ITU bed
Signs of a new intracranial haemorrhage include increasing headache, nausea, vomiting, reduced GCS, a seizure or pupil changes. These warrant urgent repeat CT head and the Alteplase must be stopped immediately until the scan is done and reported.
The CT scan show no haemorrhage. His GCS is now 10. He is on the HASU. IV fluids are started. Because he is still within the window for thrombolysis it is now restarted. He is closely monitored. A CT is booked for the following day.
8. Why is a CT scan needed the next day
9. When can Aspirin be given
10. What else do I need to check
11. The thrombolysis has finished and the patient is agitated and the BP is 210/110 mmHg. What would you do next
12. If there had been no identifiable cause for the BP rise what would you have treated him with ?
IV labetalol is the usual drug of choice in those who can take a beta blocker. It can be given as 10 mg doses which may be repeated. The key is to go slowly and avoid large drops in BP but target is to get BP comfortably under 180/110 mmHg in the 12-24 hrs after alteplase to minimise the risks of haemorrhagic transformation and bleeding into the stroke. For those who cannot take a beta blocker consider a GTN infusion though this can cause a severe headache. If the patient can swallow I might start a small dose of oral amlodipine 5 mg in addition to parenteral agents but the best advice is to follow local guidelines.
References
| PLEASE NOTE LEGAL ADVICE: The contents are under continuing development and improvements and may contain errors of omission or fact. Feedback vital and always welcome at drokane at gmail.com. This is not to be used for the assessment, diagnosis or management of patients. It should not be regarded as medical advice. It is only for educational purposes. Please adhere to your local protocols. If you are unwell please seek healthcare advice from your doctor. This does not replace senior or specialist advice. If you do not accept this then please do not use the website. If you need medical advice, please consult a doctor or other appropriate medical professional. If you are a medical professional and you need advice then speak to your senior or colleagues. |